Essays on physician and patient decision-making
Most B2C markets are relatively simple: one customer, one decision-maker, one choice. Healthcare is definitely not one of them. And the specificity, complexity, and decision stakes at play in healthcare markets have significant implications for marketing and marketers in life sciences companies.
In my PhD dissertation, I tried to unpack this by looking at the ecosystem behind patient and physician decisions. The figure below summarizes the chapters of the dissertation.
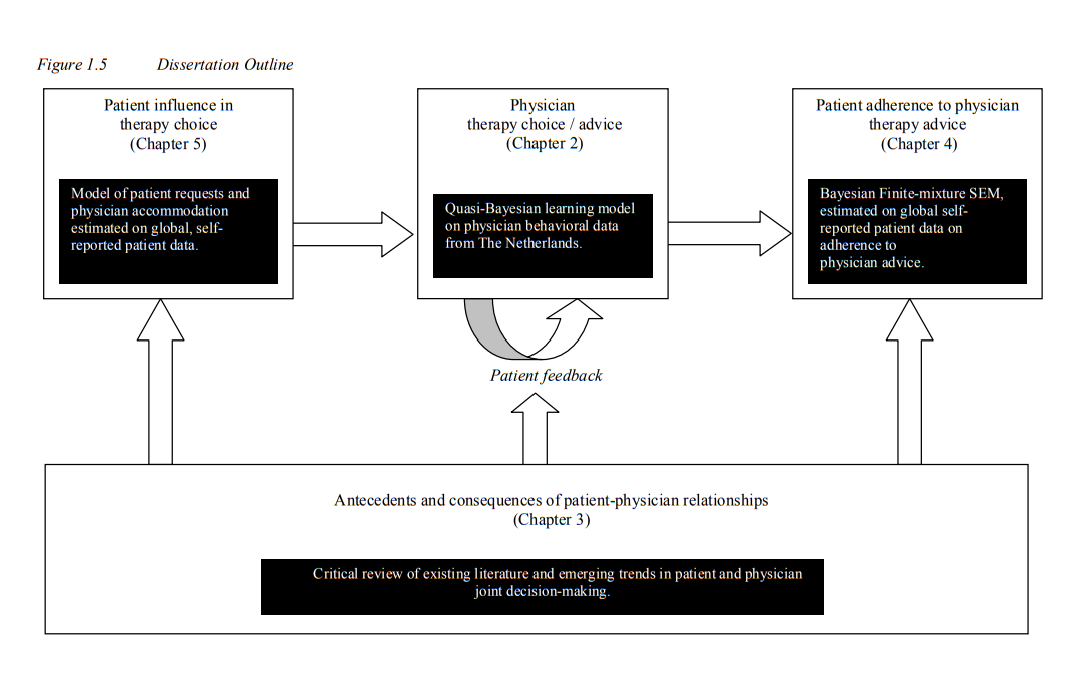
In Chapter 2, I study how physicians learn from patient feedback and how their patients’ experience with a new drug shapes their adoption and prescribing behavior over time. Using a quasi-Bayesian learning model on a very unique Dutch dataset where all GP prescriptions were recorded digitally, I examined the diffusion of AstraZeneca’s Symbicort when trying to fight the incumbent, GSK’s Seretide/Advair. The key point is simple: doctors are not, as many economists would assume, perfectly Bayesian decision-makers. Their preferences are shaped by salience effects and, thus, they overweight the feedback of a few disappointed patients. This salience effect has persistent effects through learning, habit formation and speed of diffusion of a new drug. This chapter was later published in Marketing Science.
In Chapter 3, I step back and conceptualize the joint decision-making system where patients and physicians interact and jointly make decisions. This chapter, entitled The Connected Patient has later been published in a book by Routledge Academic (Taylor & Francis), edited by Stefan Wuyts, Marnik G. Dekimpe, Els Gijsbrechts, and Rik Pieters.
In Chapter 4, the focus shifts to patients and the extent to which they adhere to physicians’ expert advice. The problem of non-adherence is well-known in healthcare: even when physicians recommend a treatment, patients do not always follow it, either because they discount the physician’s advice (reasoned non-adherence) or because they simply forget or otherwise cannot afford to follow it (unreasoned non-adherence). Adherence has tremendous consequences for patients, HCPs and pharma. In this chapter, we explore the beliefs, perceptions, and cultural context that drives adherence, with an empirical study involving more than 11,000 patients in 17 countries. This study was later published in the International Journal of Research in Marketing.
Then in Chapter 5, I close the loop: patients influence physicians as well, both through feedback and interaction (as in Chapter 2), but also through patient requests, i.e., the explicit request for a specific molecule, treatment or brand. This has implications for the patient-physician relationship, which becomes dynamic and dyadic rather than one-directional. How can physicians avoid ‘consumerism’ and ensure quality advice, while at the same time maintaining the trust and satisfaction of the patient. This is the topic of the last chapter of my dissertation.
You can read it here: https://repub.eur.nl/pub/23604/EPS2011237MKT9789058922847.pdf